Beta Cell Preservation in Type 1 Diabetes
Why Preserving Your Beta Cells Matters1,2
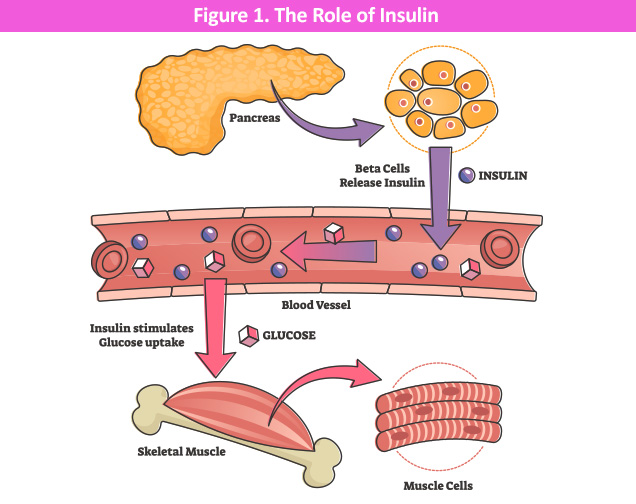
Beta cells, located in the pancreas, have a very important job, which is to produce insulin. As outlined in the figure below, insulin is like a key. It opens the doors to your body’s cells so that sugar (glucose) from the food you eat can get inside and provide energy. Without insulin, sugar stays stuck in your blood and your cells don’t get the fuel they need.
In Type 1 Diabetes (T1D), the body’s own immune system attacks and destroys these cells, which is like the factory being slowly shut down. Once most beta cells are gone, your body cannot make its own insulin anymore.
When you (or your child) are first told they have T1D, some beta cells are still alive. They are still working, even if just a little. This is called the “honeymoon period” or residual (leftover) beta cell function.
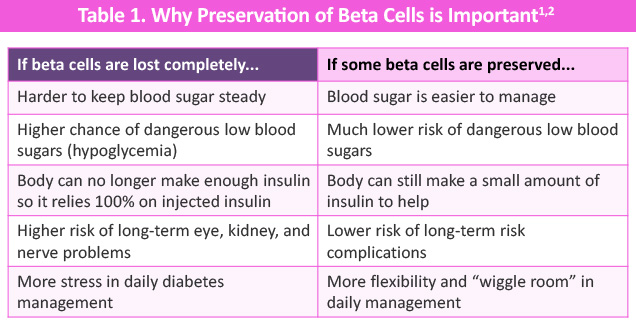
Medical research shows that keeping even a small number of working beta cells can make a BIG difference in daily life with T1D. Here is why:
Did you know?
Studies show that people with T1D who keep even a tiny bit of beta cell function have up to 65% fewer dangerous low blood sugar events.
That’s like going from getting a scary low blood sugar 10 times a year down to just 3 or 4 times.3
Why Beta Cell Function Is So Important in T1D
This is important because the difference between your body producing even a little amount of its own insulin, or none of it, can be profound.2,4 You can think of it this way: imagine you are rowing a boat across a lake. You need to get to the other side (good blood sugar control). If you have NO oars at all, it is very hard, you are pushed around by wind and waves (big blood sugar swings).
Now imagine you have just 1 oar, not perfect, but so much better! You have some control. You can steer. You can adjust. That is what a small amount of remaining beta cell function does. It acts like that 1 oar.
Even when beta cells are mostly destroyed in T1D, many people, especially soon after diagnosis, still have some working beta cells left. These cells release tiny amounts of insulin in response to food. This is called “residual” (or leftover) beta cell function.2,4
Having some residual beta cell function is important, because it can:
- Help smooth out blood sugar spikes after meals
- Protect against dangerous lows, especially overnight
- Reduce the amount of injected insulin needed
- Help the body’s blood sugar-lowering response work better overall
- Reduce the chance of a serious condition called diabetic ketoacidosis (DKA)
A real-world example from research
Scientists followed people with T1D for over 30 years in a large study (called the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications [DCCT/EDIC] study).
People who kept some beta cell function had:
- 50% lower risk of eye problems (retinopathy)
- 39% lower risk of kidney problems (nephropathy)
- 65% fewer dangerous low blood sugar events (severe hypoglycemia)
- Better blood sugar control overall (lower A1C levels)
Even very small amounts of leftover beta cell function helped—there was no level too small to make a difference!3,5
As mentioned above, in T1D, the immune system mistakes beta cells for enemies. The rate of this attack is different for everyone, typically occurring faster in children and adolescents versus adults. For most people, this can happen quietly, often for years before the first symptoms show up.
By the time T1D is diagnosed, most beta cells are already gone, but not all. Studies show that at the time of diagnosis, about 20 to 30 out of every 100 beta cells may still be alive and working.2,4
After diagnosis, the immune system usually keeps attacking. Without treatment, these remaining beta cells die off over months to a few years. This is why that window of time right after diagnosis is so important, and it may be the best chance to step in and protect what is left.
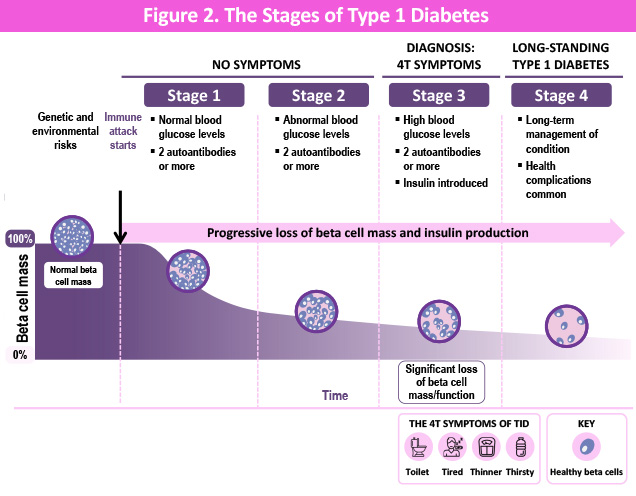
The figure below outlines the stages of type 1 diabetes. Right after a T1D diagnosis (or at stage 3 T1D), and often even before symptoms start, there is a limited window of opportunity to protect beta cells. The earlier we act, the more beta cells we can save. That’s why researches are working to find treatments early, before symptoms appear (such as teplizumab to delay progression, which you can read more about here), or other treatments being investigated to protect beta cells at diagnosis (or stage 3 T1D).
Myths and Facts—What Can YOU Do? 6,9
There is a lot of confusing information out there about beta cells and T1D. Let’s clear some of it up.
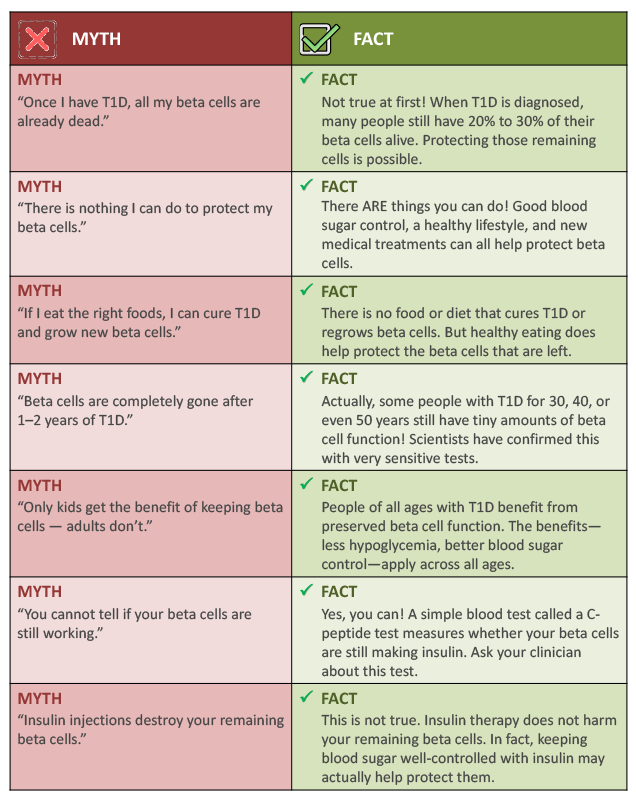
What can you do right now to help your beta cells? While there is no proven lifestyle treatment that stops the immune attack in T1D, research shows that some things can help protect the beta cells that are still alive. Here is what the evidence supports:

1. Keep your blood sugar as steady as possible.
This is the #1 thing you can do.
When blood sugar swings wildly up and down, it creates extra stress on beta cells. This is sometimes called “glucotoxicity”, which means that too much sugar in the blood is toxic to beta cells.
Good control does NOT mean perfect control. It means working with your care team to reduce big highs and lows.
Tools such as continuous glucose monitors (CGMs) and insulin pumps can help a lot.
Research from the DCCT study showed that people who used intensive insulin therapy (keeping blood sugar closer to normal) preserved more beta cell function than those on standard therapy.

2. Get diagnosed early and act quickly.
The sooner T1D is caught, the more beta cells may still be alive.
- Screening tests for T1D-related autoantibodies (the “warning signals” in the blood) can catch T1D before symptoms appear
- If you have a family member with T1D, ask about autoantibody screening programs such as ASK or TrialNet. These are often FREE
If a new diagnosis happens: Talk to your clinician right away about whether a disease-modifying treatment might be right for you.

3. Eat well and stay active.
No specific diet regrows beta cells, but overall healthy habits reduce inflammation in the body.
- A balanced diet with plenty of vegetables, whole grains, and lean protein helps keep blood sugar steadier
Regular physical activity helps insulin work better in the body (lowers “insulin resistance”).
- Aim for at least 30 minutes of movement most days, such as walking, swimming, biking, playing outside all count
- Avoid long stretches of sitting and get up and move every hour or so
4. Avoid getting sick and protect your immune system.
Infections and illness can trigger more immune system activity, which can speed up beta cell loss.
- Stay up to date on vaccines (including flu shots and COVID vaccines), since infections can make T1D harder to control
- Wash hands often
- Avoid people who are sick when possible
- Manage stress—stress hormones can raise blood sugar AND ramp up immune system activity

5. Ask about clinical trials.
The MOST powerful way to help protect your beta cells right now may be to join a clinical trial.
Clinical trials test new medicines that could slow or stop the immune attack on beta cells.
Joining a trial helps YOU and helps future generations of people with T1D.
Ask your clinician or visit Breakthrough T1D (breakthrought1d.com), TrialNet (trialnet.org), or ClinicalTrials.gov to find trials near you.
Many trials are FREE to join, and some provide travel reimbursement.
It is important to note that none of the lifestyle steps listed above replace medical treatment, and they work alongside your insulin therapy and any other treatment that your clinician recommends. Always talk to your healthcare team before making big changes.
Questions to Ask Your Healthcare Team

You (or your child) are the most important person in any conversation with your clinician or care team. Do not be afraid to ask questions. Good clinicians LOVE when patients ask questions, it means you are engaged and paying attention. Here are some important questions about beta cell preservation to bring to your next appointment. Print this page and bring it with you!
Do I (or does my child) still have any working beta cells? How do you know?
Ask about a test called a C-peptide test. This simple blood test measures whether beta cells are still making insulin. Knowing this can help guide your treatment plan and whether new therapies might help.
Is a C-peptide test right for me right now? When should it be done?
C-peptide is most useful soon after diagnosis, or when your team is considering whether to add a new type of treatment. Ask when and how often you should be tested.
Am I (or is my child) a good candidate for a disease-modifying therapy such as teplizumab?
There is now an Food and Drug Administration (FDA)-approved medication that can slow T1D progression in people who have been recently diagnosed with presymptomatic or early-stage T1D. Ask if this applies to your situation.
Are there any clinical trials we should know about?
Research on new beta cell–protecting treatments is happening right now. Your clinician may know of trials nearby. You can also ask about TrialNet, a free screening and research program for people with T1D and their relatives.
How can I tell if my beta cells are still working, and does it change my treatment plan?
Understanding your C-peptide level can change recommendations for insulin dosing, pump use, and adjunct therapies. Ask how this information will be used in YOUR specific care plan.
What blood sugar range should I aim for to best protect my remaining beta cells?
Good blood sugar control protects beta cells. Ask your care team what your personal target range should be, and what monitoring tools (such as a CGM) might help you get there.
Should my family members be screened for T1D-related autoantibodies?
First-degree relatives (parents, brothers, sisters, children) of someone with T1D have a higher risk of developing it too. Early detection can open the door to treatments BEFORE full T1D develops. Ask about options for screening, like the TrialNet or ASK programs.
What signs indicate the status of my beta cell function—whether they’re still working or have stopped?
Your clinician can explain what to watch for such as changes in how much insulin you need, blood sugar patterns, or C-peptide test results. Knowing the signs helps you stay informed.
Are there any foods, supplements, or activities I should avoid or focus on to protect my beta cells?
While no food can cure T1D, your care team can give you personalized advice on nutrition and activities that support your overall health and blood sugar stability.
Tip for your appointment
- Write your questions down BEFORE you go. It is easy to forget in the moment.
- Bring a notebook or use your phone to take notes during the visit.
- If you don’t understand something, always say: “Can you explain that in simpler words?” Good clinicians will always be happy to do this.
- You can bring a family member or friend for support and to help remember what was said.
Treatments That May Help Preserve Beta Cells10-12
Science is moving fast! For decades, the only treatment for T1D was insulin, which manages blood sugar but does not stop the immune attack on beta cells. That is changing. Here is a guide to what is available now and what is coming.
How do these treatments work?
Most beta cell-preserving treatments work on the immune system, —they try to calm down or “teach” the immune system to stop attacking beta cells. Some treatments still in development work differently: They try to actually replace the lost beta cells using stem cells.
These treatments are different from insulin. While insulin manages the symptoms (high blood sugar), these treatments try to change the root cause, or the immune attack itself, while preserving remaining beta cell function.
Teplizumab11,12
The first FDA-approved disease-modifying treatment for T1D
What is it?11,12
Teplizumab is a medicine given through an intravenous (IV, which is a tube in your arm) for 14 days in a row. It targets the immune cells (called T cells) that are attacking your beta cells. It works like a “cease fire” signal, telling the immune system to slow down the attack. It does NOT suppress the whole immune system like some other drugs do.
Possible benefits
- The first-ever medicine to change the course of T1D that is FDA-approved (approved November 2022)
- In Stage 2 T1D (before symptoms): Delayed the development of full T1D (or stage 3 T1D) by about 2 years on average (25 months) compared to those who did not get it
- In newly diagnosed Stage 3 T1D (children and adolescents, ages 8 to 17 years, PROTECT trial): Preserved more beta cell function at 18 months; patients needed less insulin and had fewer dangerous lows
- In the PROTECT trial, it was administered as 2 short courses of treatment (12 days each), separated by 6 months
- Not a daily or weekly medicine
- Does not cause long-term immune suppression
Things to know/possible drawbacks
- Given through an IV—and you will receive the medication for 14 days—at home or in an infusion center for 14 days
- Side effects can include rash, headache, diarrhea, vomiting, leukopenia, and a temporary drop in certain white blood cells (lymphopenia); most go away on their own
- Teplizumab may cause reactivation of common viruses, such as Epstein-Barr virus (EBV) and cytomegalovirus (CMV), especially in individuals with a weakened immune system. Your healthcare provider will test you for active EBV and CMV infections before treatment
- Currently approved for Stage 2 T1D (preclinical) and being studied more in newly diagnosed (Stage 3) T1D
- Does not stop or prevent the immune attack completely—it slows it down
- Expensive to access and insurance coverage may be a barrier for some families; however, patient assistance programs exist
Who might this be for?
People ≥1 year of age who have stage 2 T1D (≥2 or more T1D autoantibodies + abnormal blood sugar but no symptoms yet). Also being studied in those newly diagnosed with stage 3 T1D.
Status: FDA-approved Available now. Ask your clinician if you qualify.
Clinical trial resources and information
Learn more about clinical trials
Breakthrough T1D clinical trial information and recruitment
The big picture on new treatments11,12.
For the first time, we have a drug approved to CHANGE the course of T1D (teplizumab).
A new class of treatments is coming, including pills, infusions, and cell therapies that may someday free people from insulin injections.
The EARLIER these treatments are given, the better they work. This is why early diagnosis and screening matter so much.
None of these treatments replace insulin right now, they work alongside it.
You do not have to wait passively. Ask your clinician, join screening programs, and consider clinical trials. Researchers are genuinely close to functional cures. Your participation in research helps make it happen faster.
References
- Atkinson MA, Raghavendra MG. Cell Metab. 2023;35.9:1500-1518.
- Haller MJ, et al. Horm Res Paediatr. 2025;97:529-545.
- Diabetes Control and Complications Trial (DCCT) Research Group. Ann Intern Med. 1998;128(7):517-523.
- Fuhri Snethlage CM, et al. Diabetes Care. 2024;47:1114-1121.
- Lachin JM, et al. Diabetes. 2014;63:739-748.
- Limbert C, et al. Diabetes Care. 2023;46(10):1747-1749.
- Quick guide to type 1 diabetes (https://breakthrought1d.org.au/what-is-t1d/quick-guide-to-t1d/). Accessed 3/16/2026.
- American Diabetes Association (ADA). Diabetes Care. 2026;49:S27-S49.
- Centers for Disease Control and Prevention (CDC). Type 1 diabetes (https://www.cdc.gov/diabetes/about/about-type-1-diabetes.html). Accessed 3/16/2026.
- Participate in clinical trials (https://www.breakthrought1d.org/clinical-trials/). Accessed 3/16/2026.
- Simmons, et al. Diabetes Technol Ther. 2023;25(11):790-799.
- Ramos EL, et al. N Engl J Med. 2023;389.23:2151-2161.